Melanoma is the deadliest form of skin cancer. In Canada, there were about 9,700 melanoma cases and 1,250 deaths in 2023. Melanoma is less common among people of colour, however the mortality rate is higher. People of colour are up to 4x more likely to be diagnosed with advanced melanoma and 1.5x more likely to die from the disease. The 5-year survival rate for people of colour is 70 percent, compared to Caucasians at 92 percent.
In part, this is due to the delayed detection of cancer, with people of colour receiving a melanoma diagnosis at more advanced stages. Individuals may also be unaware of their melanoma risk or how to identify potential skin cancer lesions.
Healthcare providers can decrease the impact of melanoma by familiarizing themselves with the presentation of melanoma in people with darker skin tones and promoting melanoma awareness and effective self-exams.
Melanoma in People of Colour
Melanoma may present differently in individuals with skin of colour compared to those with fair skin, including variations in colour, morphology, and distribution of lesions.
In individuals with lower Fitzpatrick skin types, melanoma lesions with characteristic asymmetries and uneven colouration are easier to identify; lesions are also typically in places exposed to sunlight, such as the arms, back, legs, and face.
For people with higher Fitzpatrick skin types, there may be less contrast between skin colour and melanoma lesions, making it more difficult to spot colour variations and irregular borders. In addition, people with darker skin tones are more likely to develop melanoma in different parts of the body. Lesions may appear on areas with lighter skin, such as the palms of hands or soles of feet, as well as on mucosal membranes.
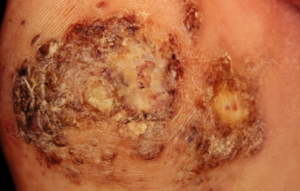
Acral Lentiginous Melanoma (ALM)
ALM is the most common type of melanoma in people with skin of colour, with a prevalence of 35-60 percent vs 2-8 percent in the Caucasian population, and is usually seen in people over the age of 40. ALM appears on the palms of the hands, soles of the feet, or beneath the fingers or toes. It begins as a flat patch of discoloured skin with variable pigmentation, resembling a bruise. Over time, it can develop into a growth or raised spot on the skin, which can become ulcerated and bleed.
ALM lesions may have distinct dermoscopic features of melanoma, including:
- A pattern of parallel ridges
- Asymmetry in both shape and colour
- Multiple pigmentation patterns across the lesion
- Pigmentation that doesn’t follow the pattern of ridges or furrows

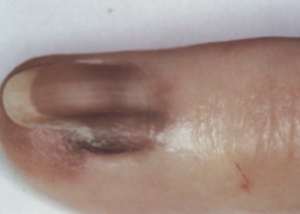
ALM occurring under the fingernails or toenails is called subungual melanoma. It typically looks like dark streaks that run vertically across the nail bed. It may be mistaken for a bruise or toenail fungus. As it progresses, it can cause the nail to break or crack.
Although ALM is the most common type of melanoma in individuals with darker skin, it is important to remember that they can still have other types of melanoma.
Mucosal Melanoma
Mucosal melanoma appears in the mouth, throat, vagina, or anus. The location of mucosal melanoma makes it difficult to identify. They may cause symptoms similar to other conditions, leading to an initial misdiagnosis. Symptoms may include:
- A mass in the affected area
- Sores or unexplained bleeding in the affected area
- Pain or itching in the affected area
Melanoma Detection
The standard diagnostic criteria for melanoma is the ABCDEF model. When examining a potential lesion, look for asymmetry, border, colour, diameter, evolution, and family history. In cases where the borders and colour of a lesion are indistinct, providers should pay special attention to changes over time. Noting the evolution of melanoma lesions can be one of the best melanoma screening strategies for people of colour. Follow-up visits and asking patients to take photos for comparison can help determine if a spot on the skin is changing in ways that suggest melanoma.
In cases of potential ALM, providers can use the CUBED model for skin lesion evaluation: colour, uncertain diagnosis, bleeding, enlargement, and delay in healing. A skin lesion that meets these criteria should be biopsied. When necessary, providers can work with oncologists and pathologists to request testing such as reflectance confocal microscopy and molecular diagnostics.
Melanoma Education
Clinicians have an important role in helping patients of colour by informing them about the risk of melanoma. It is essential to correct any outdated beliefs regarding skin cancer risks and provide a realistic overview of the risk of melanoma. Clinicians can also educate patients about ways to prevent melanoma and how to detect it early.
Patients should be encouraged to perform monthly self-exams and be reminded to check the areas of the body where melanomas are most likely to appear. Patients themselves detect 75 percent of melanomas. When possible, patients should see a doctor for an annual skin check. Ideally, patients should have the knowledge to self-advocate for an assessment of non-sun-exposed areas like the hands and feet.
Early detection of melanoma, followed by prompt treatment, improves survival rates and patient outcomes. This free, 30-minute accredited course, Melanoma in People With Skin of Colour: Diagnosis and Treatment, provides a comprehensive overview of current guidelines for early diagnosis in people with skin of colour.
Not an MDBriefCase member? Join today for free.